Hello everyone!
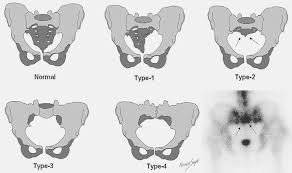
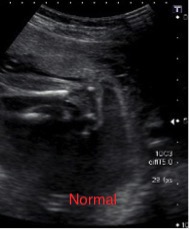
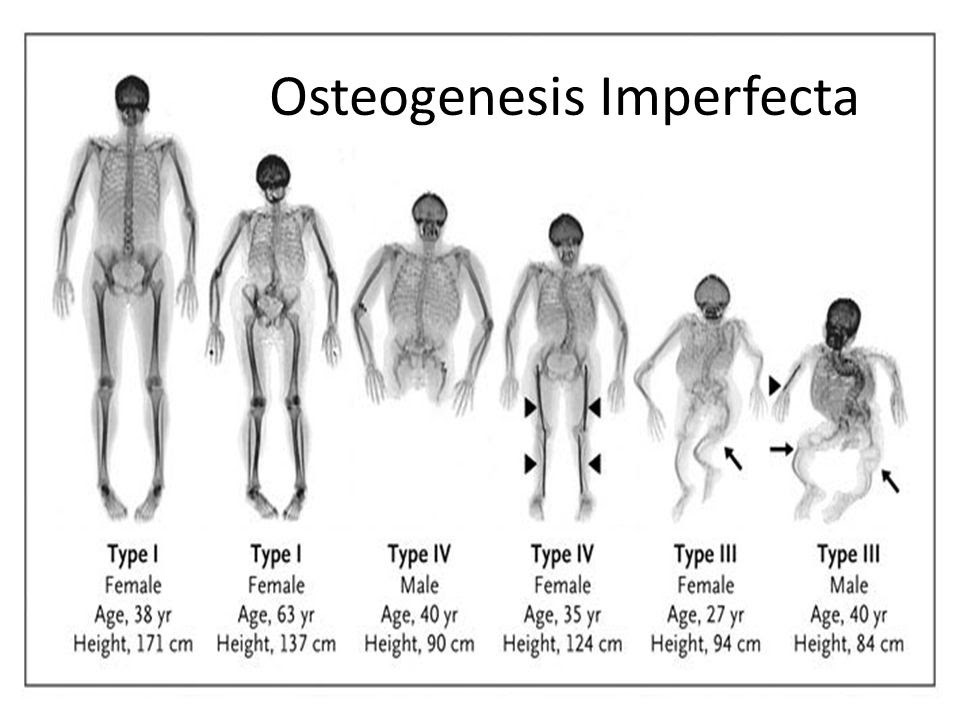
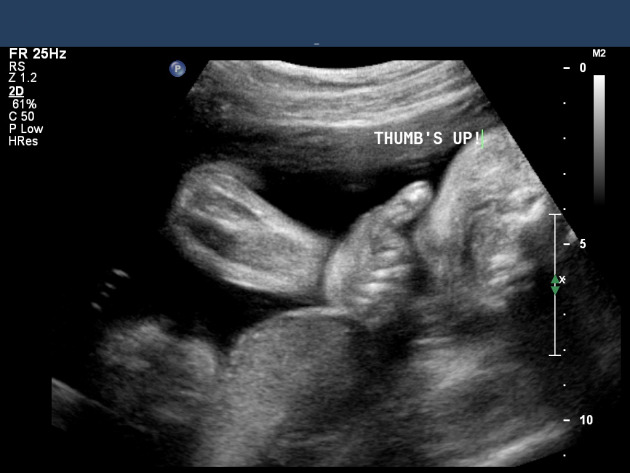
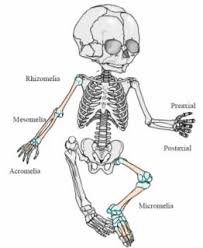
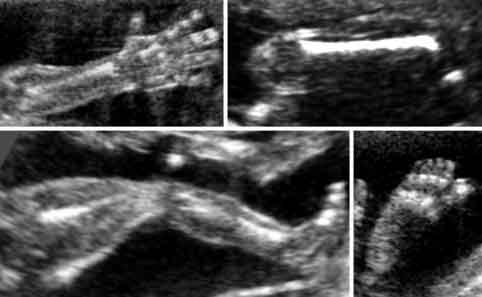
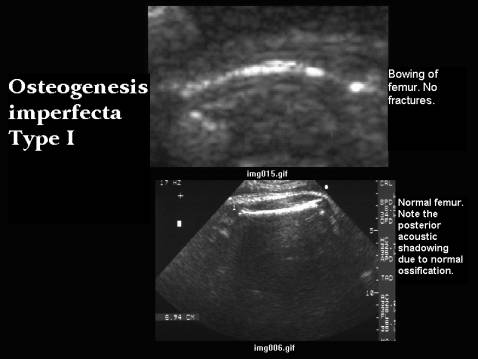
I decided to do osteogenesis imperfecta. It's a group of genetic disorders that mainly affect the bones. Osteogenesis imperfecta means "imperfect bone formation" People with this condition have bones that break or fracture easily, often from mild trauma or with no apparent cause. In this first image, it shows a comparison between the normal femur, this image shows good ossification and we know this by the shadowing thats present and no bowing with a good length. Compared to the image above that which shows type 1 osteogenesis imperfecta with bowing and it doesn't show the good ossification we see in normal.
There 8 types:
Type 1: Mildest and most common type. About 50% of all affected children have this type. There are few fractures and deformities
Type 2: Most severe type. A baby has very short arms and legs, a small chest, and soft skull. They may be born with fractured bones. They may also have a low birth weight and lungs that are not well developed. A baby with type II usually dies within weeks of birth
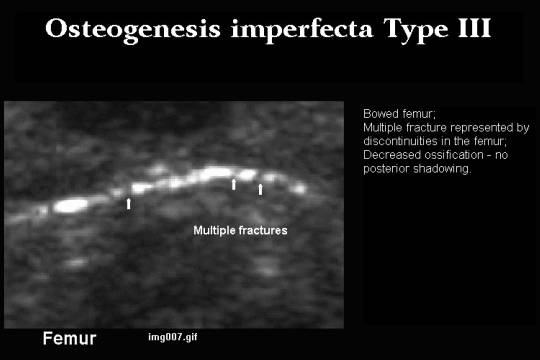
Type 3: Most severe type in babies who don’t die as newborns. At birth, a baby may have slightly shorter arms and legs than normal and arm, leg, and rib fractures. A baby may also have a larger than normal head, a triangle-shaped face, a deformed chest and spine, and breathing and swallowing problems. These symptoms are different in each baby
Type 4: Symptoms are between mild and severe. A baby with type IV may be diagnosed at birth. They may not have any fractures until crawling or walking. The bones of the arms and legs may not be straight. He or she may not grow normally.
Type 5: Similar to type IV. Symptoms may be medium to severe. It is common to have enlarged thickened areas (hypertrophic calluses) in the areas where large bones are fractured
Type 6: Very rare. Symptoms are medium. Similar to type IV
Type7: May be like type IV or type II. It is common to have shorter than normal height. Also common to have shorter than normal upper arm and thighbones.
Type 8: Similar to types II and III. Very soft bones and severe growth problems.
https://www.hopkinsmedicine.org/health/conditions-and-diseases/osteogenesis-imperfecta
379 words