So this week our reading is on multiple gestations and how this is an increased risk because of more than one fetus is occupying the womb and depending on when the cells divide will determine what kind of pregnancy this will be. Whether (Fraternal) dizygotic pregnancy versus (Identical) monozygotic pregnancy. It's also good timing since I saw my first twin pregnancy today and it was Di Di, had the twin peak sign. She used IVF so they were evaluating the babies. Super fascinating case!
Anyways, I wanted to dive into the anomalies specific to twin pregnancies to get a better handle on it, Also to ask questions about multiple gestations or any other anomalies we already discusses in the past. What I wish to get from this is more clarity and hope I help anyone along the way :) Feel free to comment!
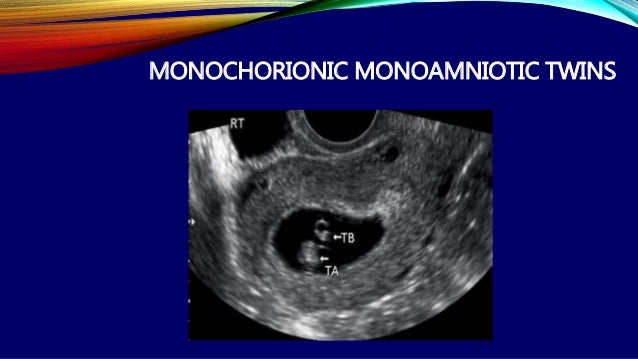
For starters of multiple gestation anomalies: (Involving all monochorionic pregnancies) Crazy right?!
-Poly -Oli sequence: I was confused by what this anomaly was and it literally tells you. Polyhydramnios and Oligohydramnios are both involved. One sac has poly while the other sac has oligo and has limited room and now stuck / smaller fetus.
-Twin to twin transfusion: Twins are discordant and aren't matching in size causing the donor to lose out on the growth.
The donor keeps giving and becomes anemic, (depleted of energy from giving) less blood flow to kidneys so not urinating = oligohydramnios.
Recipient is not used to all this generosity and gets too much blood flow to the kidneys and urinates excessively now= polyhydramnios.
With all of this receiving, fetus may get larger in size as well and go into heart failure.
Both twins are at risk for dying, why?
Answer: Donor (smaller one) is severely restricted of nutrition and oxygen rich blood supply.
Recipient (larger one) heart failure
Question: With poly-oli sequence and TTTS both affecting monochorionic pregnancies, since one is small and the other will be bigger, will they appear the same way sonographically? I tried pulling up sono images of poly-oli (stuck twin) and TTTS is the only thing that comes up.
Question: With Monochorionic: Twins are sharing one placenta correct?
Continuation anomalies...
-Twin anemia Polycythemia syndrome: Occurrences: TTTS: laser surgery is performed to clear anastomosed placenta vessels and after this surgery is can cause this dx. Its a discordance of hemoglobin: Too little hemoglobin / anemic vs too much hemoglobin / polycythemic.
-Acardiac anomaly: One develops and heart and the other doesn't. Along with no heart of upper half of the body.
-Conjoined Twins: Twins can connect at various points of their body. Occurs when the division takes place after 13 days.
-Hope someone got something out of this :)