This will most likely be a very long thread-Can each of you try to break down (in as simple of terms as possible) a cardiac pathology and explain it to the class?
Discussion Board Week 6.............
Congenital Cardiac Conditinos
Re: Congenital Cardiac Conditinos
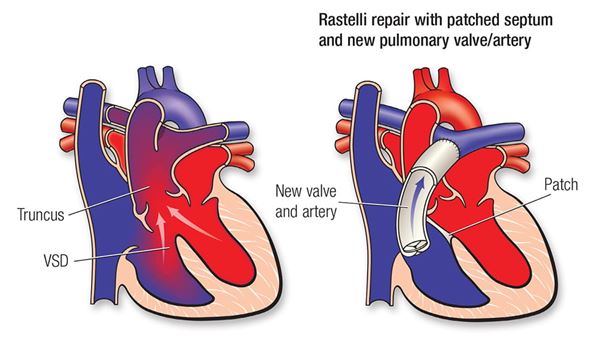
Since I missed this question on the quiz I chose persistent truncus arteriosus.
In short this is heart malformation where there is a single great artery (instead of the normal two). There will also be ventricular septal defects. This causes the oxygenated and deoxygenated blood to mix in the ventricles. Also there is no separate pathway to the lungs vs body so the mixed blood is then circulated throughout the body and sent to the lungs.
Risk factors include a diabetic mother. When blood sugars are high during early development it negatively effects heart embryolic development. There is a much higher precidence to male fetuses.
Here is the normal embryonic development, notice at 35 days there truncus arteriosus. If this fails to twist and make two great vessels it becomes persistent truncus arteriosus attached to the right ventricle.
This defect is difficult to differentiate from another deformity called double outlet right ventricle. This anomaly will have ventricular septal defects but still have a separate aorta and pulmonary artery ( although they may be difficult to see and they will both attach to the right ventricle.
This malformation will need to be corrected with surgery. The image below shows an artificial septum creating a pulmonary valve and artery.

The image below from https://sonoworld.com/TheFetus/Case.aspx?CaseId=3671&answer=1 is a post mortum image of the fetal heart at 25 weeks with severe ventricular defect and a single vessel arising from the right ventricle. The mother had no maternal risk factors contributing to the malformation.

Re: Congenital Cardiac Conditinos
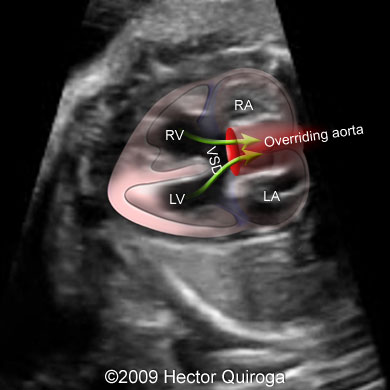
Tetralogy of Fallot:
I remember Jazmin saying it would be a tragedy to have an avatar baby with this anomaly. This anomaly causes the baby to be blue because some oxygen-poor blood is pumped to the body through the hole in the wall between the right and left ventricle instead of being pumped to the lungs. Tetralogy of Fallot is characterized by these 4 anomalies:
-pulmonary valve stenosis
-RT ventricle hypertrophy
-large ventricular septum defect
-overriding AO
TheFetus.net has amazing images showing these findings with an animation drawn over to help identify the anatomy….. ( I know I use this site a lot but it really helps me visualize these anomalies, especially difficult ones like these heart ones)





We usually don’t see the hypertrophy of the RT ventricle until later on in the pregnancy when the musculature of the fetal heart is more developed and easier to visualize.
Re: Congenital Cardiac Conditinos
Love thefetus.net! I think of tetris, and with tetralogy of fallot all four pieces have to fit. except for the right ventricular hypertrophy since in utero mom is still doing the work for baby. Once the baby is born and is responsible for moving it's own blood that right ventricle becomes effected.
Re: Congenital Cardiac Conditinos
Ooh thanks Heather! I like the tetris analogy. After talking about these heart anomalies I have been scanning a lot of 3rd trimester growth exams. I can clearly see the heart muscle with these little ones since they are a lot further along. I wonder when following babies with Tetralogy of fallot we will eventually see the right ventricular hypertrophy?
Re: Congenital Cardiac Conditinos
Hello Amanda,
I love the last picture of the overriding aorta. it took me a while to understand what that term meant exactly. Now I understand a overriding aorta is pulling blood from The right ventricle and the left ventricle. Also a great job listing the four characteristics of Tetralogy of fallot.
Re: Congenital Cardiac Conditinos
hey guys, I want to share a chart that I saw at my clinic hopefully it helps you guys!
Re: Congenital Cardiac Conditinos
Hi Lauren,
This is amazing thank you. So the first one is "patent ductus arteriosus". This confused me at first because I thought that patent meant it is functioning properly. I was reading the indication underneath the picture and it and it says that its when the ductus arteriosus doesn't close after birth.....is that correct? On a side note, I'm sure this is found after baby is born and since it is a cardiac anomaly, would cardiac sonographers see this patient and take images of the heart, or will general, genetics, or perinatology sonographers examine this patient?
Re: Congenital Cardiac Conditinos
The anomaly I would like to elaborate on is TAPVR Total anomalous pulmonary venous return. This is one of the anomaly that focuses on the pulmonary veins. I learned from the reading that you can either have partial anomalous pulmonary venous return or total anomalous pulmonary venous return.
With total anomalous pulmonary venous return: all of the pulmonary veins are going from the superior vena cava into the right atrium normally the pulmonary veins should drain into the left atrium. This Causes the oxygen rich blood to mix with the Deoxygenated blood and shunt fetal development and growth.
With partial anomalous pulmonary venous return some of the pulmonary veins are going into the left atrium and some of the pulmonary veins are going into the right atrium. Partial anomalous pulmonary venous return is not as severe effects as total because the fetus still get some oxygen rich blood. With partial anomalous venous return it is more common to have an abnormal connection from the right lung.
https://www.cdc.gov/ncbddd/heartdefects/tapvr.html

Re: Congenital Cardiac Conditinos
Reading through this anomaly again it makes sense that if its partial its typically from the right lung. So the left lung connects correctly to the left atrium and then the right pulmonary veins don't make it all the way across to the left and instead attach to the right atrium.
As a beginner with fetal heart images knowing that this type of detailed anatomy can go wrong is scary. I still have to work hard for the 4ch, LVOT, RVOT, and septum that we take at our site. It's good to be aware that even if the big picture items are placed correctly that these hard to visualize pulmonary veins can misroute.